


Introduction
Not everyone requiring treatment for a damaged or diseased bladder receives a urostomy. For some people, a neobladder is more suitable. If you’ve been told this is an option for you, you’re bound to have lots of questions.
Here are answers to some commonly asked questions:
What is a neobladder?
A neobladder is a general term applied to a specific type of bladder reconstruction.
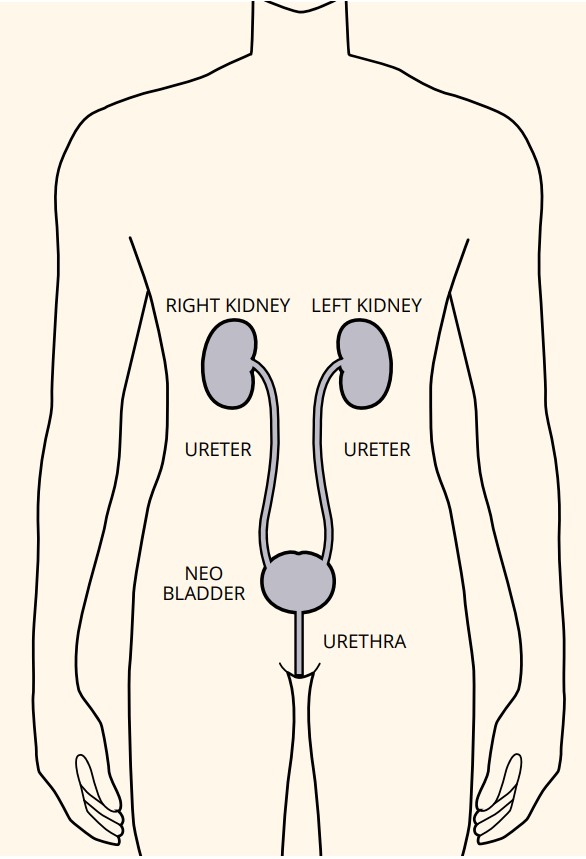
Your surgeon will aim to construct the neobladder by using a piece of your bowel. This piece of bowel is reshaped to create a functional reservoir for your urine. The neobladder is then connected to your:
- ureters (the tubes that drain urine from your kidneys) at the top
- urethra (the tube that takes urine out of your body) at the bottom
Because the surgery for a neobladder takes longer and is slightly more complicated than that for a urostomy, it is likely to involve a longer stay in hospital afterward.
How will I know if I am suitable for a neobladder?
There are three primary considerations:
- Is everything else working as it should? – The main consideration is whether you will have a functioning urethra and urethral sphincter after your cystectomy. A neobladder would not normally be an option if your urethra has disease (e.g. stricture, sphincter-weakness or cancer).
- Your quality of life after surgery – If you do have a functioning urethra, the next consideration is physical fitness. Having such a complex surgery can take its toll on your body. A urostomy might be more suitable for you to ensure you have the best quality of life after your surgery.
- The extent of your condition – Due to the extent and or exact location of your condition, a neobladder may be not suitable; this is something that your surgical team explain to you.
Other factors that a surgeon will take into consideration:
- Age (usually under 75 years of age)
- General health and fitness
- Motivation (how motivated someone will be to spend time training their neobladder)
- Expectations:
- Is the individual prepared to tolerate a degree of urinary incontinence, particularly at night (affecting approximately 3 in 10 people)
- Is the individual prepared to self-catheterise should they develop excessive or abnormal continence (affecting approximately 1 in 10 people).
What is surgery like for a neobladder?
When surgeons perform a cystectomy with the intention of forming a neobladder, they will usually attempt to keep as many of the nerves intact around the area of bladder. This has the added benefit of preserving sexual function in some people, particularly women.
Once the cystectomy is complete, the surgeon will fashion your neobladder using a section of your bowel. You may experience a short period of altered bowel habit afterward, but this is normally temporary.
When you wake up after a cystectomy and neobladder formation, you’ll have several tubes attached to your body. These are perfectly normal and are there to help reduce the risk of complications. These include:
- a urethral catheter
- a tube on your lower tummy that goes directly into the neobladder. This is called a suprapubic catheter.
- ureteric stents – thin tubes that drain urine from your ureters
- a wound drain
You’ll stay in hospital for up to three weeks after surgery. Initially the tubes will need to be flushed by nursing staff – probably three or four times a day.
Before the catheters are removed, you’ll need an Xray (cystogram) to ensure that the internal sutures have healed. This is usually carried out between 10 days and two weeks following surgery. Once this healing is confirmed, your urethral catheter will be removed, followed by the suprapubic catheter. These are usually removed at the same time; however some patients will be discharged with one or both of the catheters still in place, and have them removed during an outpatient appointment.
What is it like living with a neobladder?
It takes a while to get used to a new bladder and learning how to look after it. Like anything new, it will get easier with time and practice. Your nurse will be there to support you before and after your operation.
The bowel tissue used to make your neobladder will continue to produce mucus, which might appear as pale threads in your wee. Although this is not a problem for most people, about one in 20 patients find that excessive mucus is causing urine retention or infections. In this case, they might need regular ‘flushing’ of their neobladder. Again, your nurse will teach and support you in learning how to do this.
It is natural to feel anxious about going out in public and to worry about finding a toilet in time. It helps to plan ahead, because being prepared can help you feel more confident.
What will I need when I return home after surgery?
Most people don’t need to be prescribed any particular equipment, although you will probably want to get some protective sheets.
You will be given the phone numbers of who to contact for advice once you’re back at home. The teams are there to support you, so do ask for their help with any questions or difficulties you may have
How will I wee with a neobladder?
The initial few weeks are critical while you train your new bladder both to hold urine and empty it when required. Most neobladders hold a very small volume to begin with, but they gradually expand to hold more urine as time goes on.
There are several ways to train your new neobladder. These are:
- delaying emptying your bladder by contracting and strengthening your pelvic floor to increase your neobladder capacity
- sitting to pass urine (both men and women)
- learning to relax your pelvic floor at the same time as gently straining down to empty your neobladder.
With time and practice, most people learn to empty their new bladder in the same way as before their operation, by weeing into the toilet. Men and women will have to sit to empty their bladder, and you’ll usually have to strain or apply gentle pressure with your hands over your lower tummy to start with.
At first, you will have to empty your bladder every hour or so. The feeling of needing to wee will be different from before your surgery and you will learn to identify the new sensations which tell you that your bladder is full.
Over time, your new bladder will stretch and be able to hold more urine. But you may still have to empty it every four hours. You may also need to use a catheter a few times during this period. This helps to ensure your new bladder is completely empty. If you need to do this, your nurse will show you how.
However, if you have difficulty passing urine in this new way over time, you might need to use a catheter to empty your new bladder on an ongoing basis. Again, your nurse will support you with this.
Will I experience leakage of wee?
Early on, you might experience some leakage, particularly at night. Rest assured; this usually gets better after a few months. Your nurse can suggest things to help and may refer you to a continence adviser.
Your nurse will teach you how to do pelvic floor exercises. It is important to keep doing these as they can help you have more control over leakage.

- This information is available as downloadable leaflet. Visit our ‘leaflets and downloads‘ page.