


What is an internal pouch (also known as a continent urinary diversion or Mitrofanoff)?
If your bladder doesn’t work or is removed, you’ll need another way to pass wee. Known as a urinary diversion, there are several ways of doing this, including:
- Urostomy – an opening on your stomach that lets your wee drain out, into a bag
- Bladder reconstruction (neobladder) – where a surgeon creates you a new bladder from a section of your bowel
- Nephrostomy – when an opening is made on your back so urine can drain straight from your kidneys
- Continent urinary diversion (also known as an internal pouch or Mitrofanoff ) – when a section of your bowel is used to create a new internal pouch, which is drained using a catheter.
You can discuss with your surgeon what urinary diversion options might be best for you. They might suggest an internal pouch if:
- you are unable to, or don’t want to have, a bladder reconstruction (neobladder)
- you want to avoid wearing a urostomy bag to collect your wee
- your risk of the cancer coming back is low
- your bowels are working well and aren’t affected by any other problems, such as Crohn’s disease or previous bowel surgery
- you haven’t had – and won’t be having – radiotherapy to your pelvis
- your liver and kidneys are working well
- you are willing and able to learn how to pass a thin tube (catheter) into your stoma (self-catheterisation).
If you’re considering an internal pouch, you’ll need to be highly motivated as it takes time to train it, and you will need good dexterity to use the catheters.
The operation to create an internal pouch is more complex than a urostomy, and around 20% of people need further surgery to correct problems afterwards. Your consultant will explain the risks as well as the benefits so that you are prepared for what might happen and can ask questions.
How an internal pouch is made
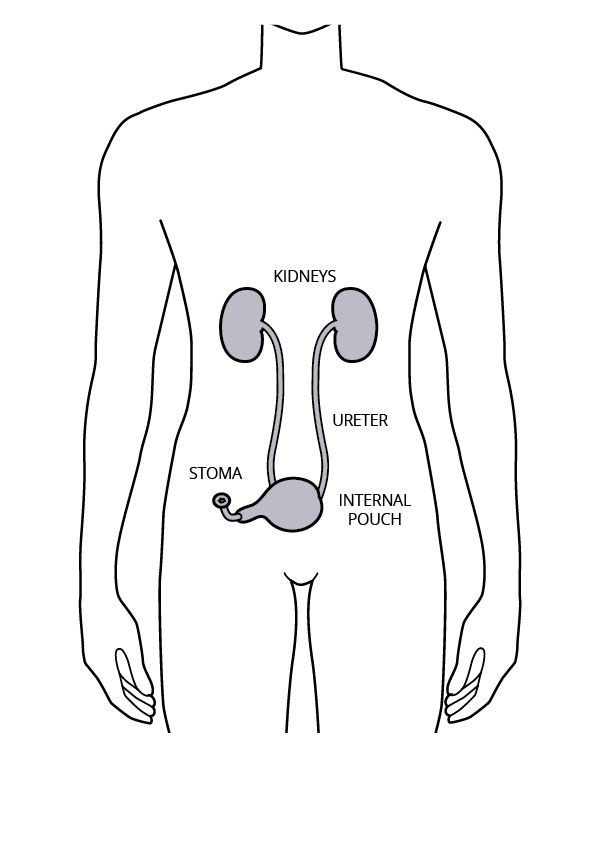
During the operation to remove your bladder, your surgeon will create your new internal pouch using a section of bowel. They sew the tubes that carry urine from your kidneys (ureters) to the pouch so that your wee runs down the ureters, into the pouch.
The other end of the pouch is connected to a small opening on your tummy, called a stoma. Your surgeon will create your stoma at – or just underneath – your tummy button so that it won’t show under your clothes.
A natural valve keeps the stoma closed so that wee doesn’t leak out.
Your nurse will teach you how to drain the pouch using a catheter. This enables you to be continent and in control of when you empty your pouch. For most people, this is every five or six hours.
Before surgery
This is major surgery and investigations such as blood tests, chest x-ray, electrocardiograph and a kidney scan or an x-ray may be performed. You will be admitted the day before surgery and if your surgeon may request some bowel preparation to clean out the bowel beforehand.
After surgery
You’ll usually stay in hospital for 5–7 days.
When you come round from surgery, you will have several tubes attached to you. Don’t be alarmed – they are part of your treatment. You’ll receive pain relief to help you feel comfortable and intravenous fluids to keep you nourished as you gradually return to a normal diet.
You are likely to have a drain from your abdomen, to get rid of excess fluid from the operation site. A large drainage tube will drain the new internal pouch, which will be irrigated several times a day to prevent any blockage.
Two fine tubes (known as “stents”) will also be inserted alongside this tube. These will be removed after about ten days. The two catheters (one going into your pouch through your tummy and one going through your stoma) stay in place for a few weeks while you recover from your operation.
Drink plenty, eat small amounts often, and rest—you may feel tired at first.
Once the pouch has healed, which typically takes around six weeks, you will go back to the hospital. You will usually stay there for one or two days for the catheters to be removed.
Caring for your new internal pouch
Before you leave hospital, your specialist nurse will make sure you have a supply of the things you need, including catheters. Once home, you can get your equipment free on prescription directly from a supplier or your pharmacy. Your nurse will explain all this.
When you return home, you will still be able to ask your specialist nurse for advice. The hospital will arrange for a district nurse or a community stoma nurse to visit you when you first leave the hospital. They can help you manage any difficulties.
At first, your stoma will look swollen and red, but it won’t hurt because it has no nerve supply. It will gradually shrink as it heals and becomes less noticeable.
You don’t need to cover the opening unless it gets sore. It doesn’t need to be covered when you bathe, shower or swim either, though some people choose to put a waterproof dressing over it. If the area becomes irritated, or it leaks or bleeds, contact your GP or nurse specialist for advice.
Some blood in your wee is normal at first, but speak to your nurse if you’re worried.
Emptying your pouch
To empty your pouch, you put a catheter through your stoma into the pouch. Your specialist nurse will teach you how to do this. At first, you’ll need to do it every one to two hours, until your pouch stretches.
With time, you may be able to leave your pouch for up to six or seven hours before emptying it. It can be helpful to set an alarm to remind yourself to do this.
If you experience trouble inserting a catheter, try pulling it back a bit and gently pushing it in again. Try rolling the catheter between your fingers as you put it in.
Night drainage
At first, you’ll leave a catheter in place overnight, and this will be connected to a night drainage bag. Eventually, you may find that if you reduce how much you drink a couple of hours before bedtime, and completely empty your pouch just beforehand, you can sleep as normal without a catheter. If you drink lots in the evening or find that your pouch fills overnight, consider setting an alarm to wake you so you can empty your pouch.
Washing out your pouch
As well as emptying your pouch, you need to wash it out. The pouch is made from a piece of bowel, which means it doesn’t behave exactly like a bladder. The bowel produces mucus, which can build up in the pouch if not washed out, putting you at risk of infection.
You do it by putting fluid through the catheter that you use to drain the pouch. Your surgeon or nurse will advise you how often to wash out your pouch.
Living with a continent urinary diversion
Looking after your pouch takes time to learn, but it gets easier.
Be sure to drink lots of water to help avoid urinary tract infections (UTIs) and irritation. Aim for two to three litres of fluid a day.
It is natural to feel anxious about going out in public and to worry about finding a toilet in time. It helps to plan ahead because being prepared can help you feel more confident.
For travel, take extra supplies and a letter from your GP.

Follow up
Your consultant will make arrangements for your check-ups. These will be more frequent initially, but then usually once a year. You’ll probably have a blood test to check your kidney function and every few years you might need a kidney scan or x-ray.
Annually, you’ll need a:
- blood test to monitor serum biochemistry including bicarbonate and chlorides, blood count and eGFR (estimation of Glomerular Filtration Rate, a test to monitor kidney function).
- blood pressure check
- renal ultrasound (kidney scan).
Urinary tract infections (UTIs)
If your wee becomes cloudy and offensive smelling and you have flu-like symptoms with pain in your kidney area and abdomen, it may be due to a urinary tract infection.
Contact your GP and collect a urine specimen from your pouch using a sterile catheter. You need to ensure that a note is put with the specimen saying that it is from a continent diversion.
Recurrent UTIs can be caused by incomplete emptying of your pouch, perhaps because your catheter is becoming blocked by high levels of mucus. Calculi (stones) in the pouch may also be the cause. Your GP may refer you back to your Consultant for further investigations, if infections persist.
Discharge
If your bladder was not removed, you may get discharge. See your GP if it’s painful or smelly.
Do you want to speak to someone?
Many people who contact the Urostomy Association tell us that following surgery for a urinary diversion, that they have returned to an active and rewarding lifestyle. We often hear them describe it as ‘restoring their quality of life’. If you’d like to speak to a Urostomy Association buddy with personal experience of a urinary diversion, please contact the office and we’ll put you in touch.
- Huge thanks to Paul Russell-Roberts, Stoma Care Nurse Specialist, for reviewing this information page


